Your oncologist mentioned a treatment that does not involve drugs or radiation. They called it tumour treating fields. They said it uses electrical fields to slow cancer growth. They said you wear it on your body. You went home unsure whether this is real medicine or science fiction.
It is real medicine. Tumour treating fields, often abbreviated TTFields and sold under the brand name NovoTTF, is FDA-approved for pleural mesothelioma. This guide explains how it works, who it is for, what wearing the device is actually like, and what survival data has been reported.
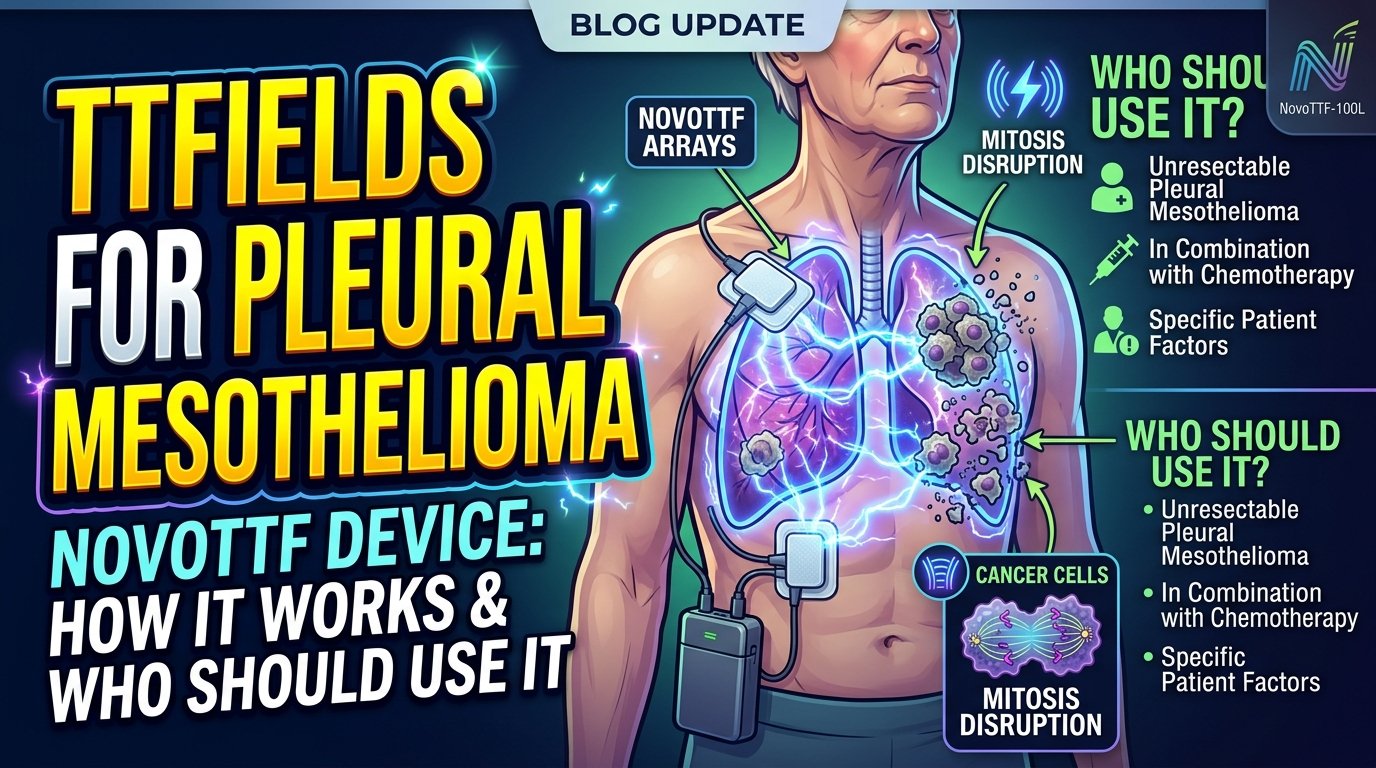
TTFields therapy is delivered through transducer arrays worn on the chest skin.
How TTFields Work
Tumour treating fields use low-intensity, alternating electric fields to disrupt cancer cell division. When a cell divides, certain molecules inside the cell need to align in specific ways to complete the division. The alternating electric fields interfere with this alignment. Cancer cells, which divide much more frequently than healthy cells, are disproportionately affected.
The fields are generated by a portable device the patient wears. Adhesive patches called transducer arrays are placed on the skin of the chest, four arrays per session, and connected by wires to the generator carried in a small bag. The patient wears the device most hours of the day, ideally eighteen hours or more, with brief breaks for showering or skin care.
FDA Approval for Pleural Mesothelioma
The FDA approved TTFields for unresectable pleural mesothelioma in 2019. The approval was based on the STELLAR trial, which combined TTFields with standard chemotherapy and showed median survival improvement compared to historical chemotherapy controls. The approval is for use in combination with first-line chemotherapy in patients who cannot have surgery.
The device is also approved for glioblastoma brain cancer and pancreatic cancer in the United States. The same underlying technology, with different field configurations, is used for each indication. The mesothelioma version is specifically tuned to the body region and tumour location involved.
TTFields is added to standard chemotherapy for unresectable pleural mesothelioma.
What Wearing the Device Is Like
The transducer arrays are placed on the chest by a trained technician at the start of treatment. The skin underneath needs to be clean and shaved. Patients shave their chest hair every few days to maintain good contact. The arrays are replaced every two to four days as the adhesive wears out and the skin needs care.
The generator is about the size of a small handbag. It runs on rechargeable batteries that last approximately three to four hours each. Patients carry spare batteries and swap them throughout the day. The device makes a quiet electronic hum but is otherwise unobtrusive. Most patients can continue normal activities with the device on, including light exercise.
The most common side effect is skin irritation under the transducer arrays. Mild redness, itching, and occasionally blistering can develop. Skin care with topical steroids and array repositioning manages most cases. Discontinuation due to skin issues is uncommon when the team is experienced.
Who Is a Candidate
The FDA approval covers patients with unresectable pleural mesothelioma who are starting first-line treatment with chemotherapy. The device is used in combination with chemotherapy, not as a replacement. Patients who are surgery candidates are typically directed to surgery rather than TTFields.
Patients with implanted electronic devices like pacemakers cannot use TTFields because of potential interference. Patients with skin conditions that prevent secure adhesion of the arrays may have difficulty using the device effectively. Patients who cannot tolerate wearing the device for long periods may not benefit because adherence under eighteen hours a day reduces the treatment effect.
Survival Data and Cost
In the STELLAR trial, the median survival with TTFields plus chemotherapy was approximately eighteen months, compared to historical chemotherapy controls of approximately twelve months. The improvement was meaningful, particularly given that there was no increase in chemotherapy-related side effects. Long-term follow-up has continued to show survival benefit, with some patients exceeding three years of survival on the combination.
The device is expensive. The monthly cost approaches twenty thousand dollars before insurance. Coverage varies by plan. Networks behind major commercial insurers and Medicare typically cover the device when used for FDA-approved indications, though prior authorisation is required and the process can be lengthy. The manufacturer, Novocure, has patient support programmes that help with insurance navigation and financial assistance.
Practical Considerations
TTFields is a commitment. Wearing the device eighteen hours a day for many months requires lifestyle adjustment. The visible nature of the device makes hiding the diagnosis from coworkers or social contacts impossible. The skin care, battery management, and array changes become a daily routine.
For patients who can adhere to the protocol, the survival benefit appears real. For patients who cannot or do not want to wear the device consistently, the treatment effect is diminished. The decision should be made with eyes open about the practical demands.
Combining TTFields With Newer Therapies
Trials are now testing TTFields combined with immunotherapy as well as chemotherapy. The mechanisms are independent and may produce additive effects. Early results are encouraging but the formal data is still maturing. Patients on first-line immunotherapy who are interested in adding TTFields should ask their oncologist whether off-label use is appropriate or whether trial enrolment is an option.
The integration of TTFields into broader mesothelioma treatment protocols is still evolving. The next several years will likely see expanded combinations and clearer guidance on when the device adds the most value.
A Closing Note
TTFields represents a fundamentally different approach to cancer treatment than drugs or surgery. The mechanism is novel. The evidence is real. The practical demands are significant. For unresectable pleural mesothelioma patients who can adhere to the wearing schedule, the device offers a meaningful additional tool alongside chemotherapy.
Ask your oncology team whether TTFields is an appropriate addition to your treatment plan. The answer depends on your tumour, your overall treatment strategy, and your willingness to commit to the protocol. The conversation is worth having explicitly rather than assuming the device is or is not relevant to your case.
This article is for educational purposes and does not replace personalised guidance from a medical oncologist.
Your local hospital has an oncology department. They can give you chemotherapy. They can do basic surgery. They have managed cancer patients for decades. But they have probably never seen a mesothelioma case before yours. This is normal. Mesothelioma is rare. Local oncologists may diagnose it once or twice a year, sometimes never.
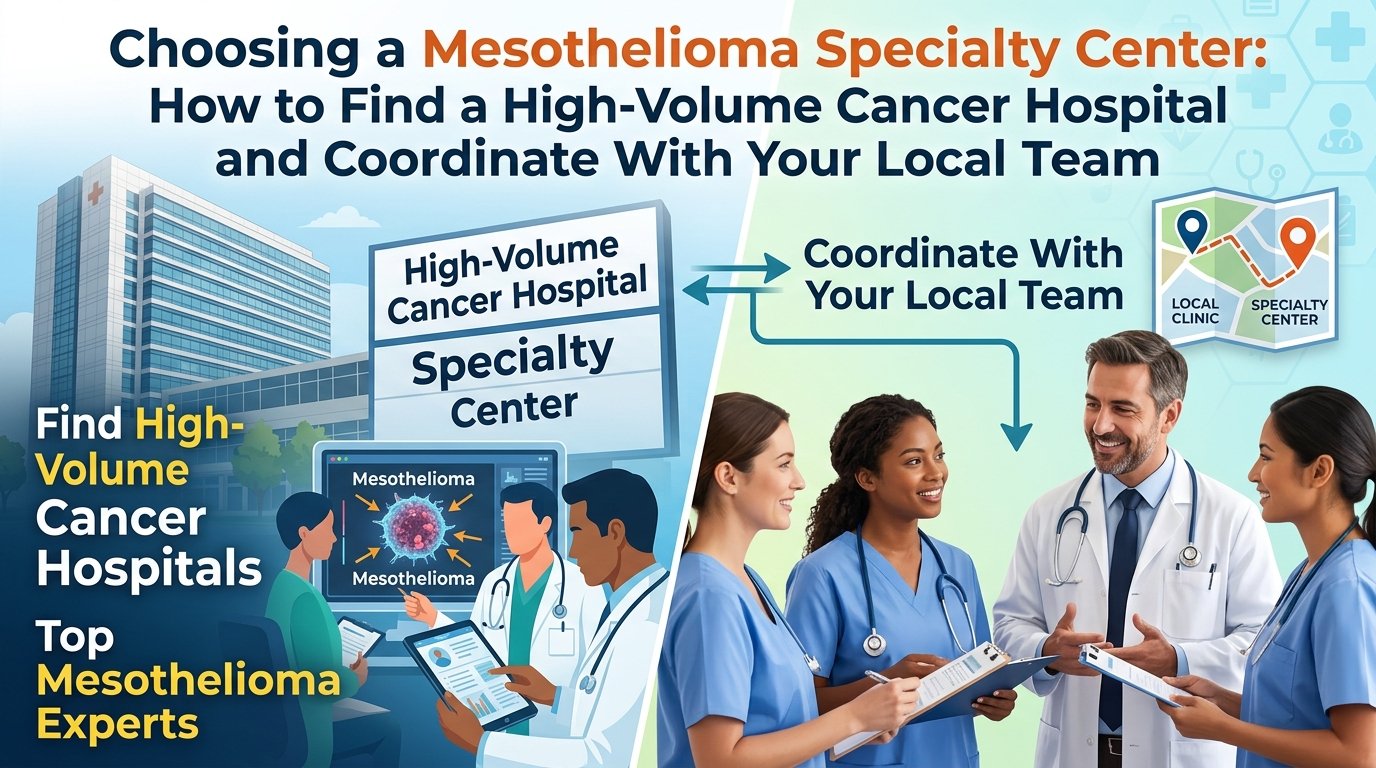
The decision of where to receive your mesothelioma treatment is one of the most consequential decisions in your care. Outcomes at high-volume specialty centres are measurably better than at general oncology practices for this disease. This guide explains how to find a specialty centre, what to expect when you go, how insurance handles travel for treatment, and how to integrate specialty care with your local team.
Mesothelioma specialty centres are concentrated in major academic medical centres.
Why Volume Matters in Mesothelioma
Surgical and oncology outcomes for rare cancers consistently track with the volume of cases that the centre and the individual physicians handle. For mesothelioma, the volume effect is particularly pronounced. Surgical mortality, complication rates, completeness of cytoreduction, and median survival all favour high-volume centres. The differences are not small. They are clinically meaningful.
The reasons are straightforward. High-volume centres have surgeons who perform many cases per year, oncologists who follow the latest mesothelioma-specific evidence, pathologists who can confirm rare diagnostic findings, radiation oncologists experienced with mesothelioma planning, and supportive services that have managed the specific complications of the disease. The infrastructure cannot be replicated in a centre that sees mesothelioma rarely.
The Major Centres in the United States
Several mesothelioma treatment centers have established multidisciplinary programmes with high volumes and strong outcomes. The list is not exhaustive but includes the National Cancer Institute, the Brigham and Women’s Hospital International Mesothelioma Program, the University of Pennsylvania, MD Anderson Cancer Center, Memorial Sloan Kettering Cancer Center, the University of Pittsburgh, the University of Chicago, the Pacific Mesothelioma Center, the Baylor College of Medicine programme, and several others.
Each programme has slightly different specialties. Some lead in surgical innovation. Some lead in clinical trials. Some specialise in peritoneal disease. The Mesothelioma Applied Research Foundation maintains a directory of programmes that can help you identify centres that are reasonable matches for your specific case.
Specialty centres offer multidisciplinary teams not available at most local hospitals.
What to Expect at a First Visit
A first visit at a specialty centre typically involves a half-day to full-day commitment. You will see multiple specialists in sequence: a thoracic surgeon, a medical oncologist, a radiation oncologist, sometimes a pulmonologist, and supportive services. Each will review your case in detail and contribute to a coordinated treatment plan.
Bring all your medical records, imaging on a CD or via electronic transfer, pathology slides if possible, and a list of every medication you take. The centre will often request that pathology slides be sent in advance for review by their own pathologists. A confirmed diagnosis is the foundation of treatment planning, and second-look pathology occasionally changes the diagnosis or refines the cell-type classification.
Expect to leave with a written treatment recommendation, a sense of timing for treatments and follow-ups, contact information for ongoing communication, and a clear plan for how the centre will coordinate with your local oncologist for routine care between specialty visits.
Travel and Lodging Logistics
Most patients receiving care at a specialty centre live some distance from the centre. Travel becomes part of the treatment plan. Major centres have patient navigators who can help with logistics including flights, hotel discounts, and patient lodging programmes that provide low-cost accommodation near the hospital. Hope Lodge from the American Cancer Society is one such programme operating near several cancer centres.
For surgery and inpatient stays, family members typically travel with the patient. The Joe Andruzzi Foundation and similar organisations provide grants for travel costs. Some airlines offer compassionate fare programmes. Hospital social workers can help identify resources specific to your situation.
Insurance and Out-of-Network Care
The specialty centre may not be in your insurance network. Out-of-network care is often covered when the procedure is medically necessary and not available locally. The key is documentation. The specialty centre’s case management team handles the prior authorisation process, working with your insurance to obtain approval for treatment as a single-case agreement or out-of-network exception.
Approval is usually granted for mesothelioma cases because the disease is rare and the volume effect is documented. If approval is initially denied, appeal. Specialty centres have appeals teams experienced in mesothelioma authorisations. The first denial is often reversed on appeal with appropriate clinical documentation.
Coordinating With Your Local Team
Going to a specialty centre does not mean abandoning your local oncologist. The most common arrangement is a hub-and-spoke model where the specialty centre directs the overall plan and the local team delivers routine chemotherapy infusions, monitors blood work, manages day-to-day side effects, and provides follow-up care between major visits.
This arrangement preserves continuity of care, reduces travel, and uses each team’s strengths. The specialty centre brings deep mesothelioma expertise. The local team brings familiarity with you, accessibility, and integration with your other healthcare. Communication between the two teams should be explicit, with shared records and regular updates.
Second Opinions Are Standard
Even after establishing care at one specialty centre, second opinions at other centres are reasonable for major decisions like surgical approach, eligibility for clinical trials, or transitions between lines of therapy. Most specialty centres expect and welcome second opinions. The patient’s confidence in the chosen plan is part of the treatment, and second opinions reinforce or refine that confidence.
Insurance generally covers second opinions for cancer treatment. The specialty centres have streamlined the process. Bringing your records to a second consultation does not commit you to changing your care; it informs your decision.
A Closing Recommendation
If you have been diagnosed with mesothelioma, prioritise getting a consultation at a high-volume specialty centre early. The travel is worth it. The expertise is worth it. The connection to clinical trials and the latest treatment approaches is worth it. The local relationship can continue alongside specialty care, but the specialty foundation should be in place from the start.
Ask your local oncologist for a referral. If they hesitate, advocate for yourself. The Mesothelioma Applied Research Foundation, Mesothelioma Hope, and patient advocacy organisations can help with referrals. The first step is the appointment. The rest unfolds from there.
This article is for educational purposes and does not constitute personalised medical advice.
You went to the doctor short of breath. They listened to your chest. They sent you for a chest X-ray. The X-ray showed fluid around your lung. They drained the fluid. They tested it. Mesothelioma cells were present.
This is how many mesothelioma diagnoses begin. The fluid is called pleural effusion. It is one of the earliest and most consistent signs of pleural mesothelioma. This guide explains what causes pleural effusion in mesothelioma, how it is drained, what the drainage reveals, and what role recurrent effusions play in long-term symptom management.
The pleural space normally contains only a thin film of fluid; mesothelioma causes large effusions.
What Pleural Effusion Is
The pleural space is the thin gap between two layers of tissue that line your lungs and your chest wall. Normally this space contains only a few teaspoons of lubricating fluid. The lung slides easily against the chest wall during breathing. When mesothelioma develops on the pleural surfaces, the affected tissue produces excess fluid. The fluid accumulates in the pleural space, sometimes in volumes of one to several litres.
The fluid compresses the lung. Less air can enter. The patient experiences shortness of breath that worsens with activity, a feeling of chest fullness, and sometimes pain. As the effusion grows, even minimal exertion produces breathlessness. The fluid is the symptom that often drives the first diagnostic workup.
How Effusions Are Drained
The first drainage is usually a thoracentesis. A thoracentesis is an outpatient procedure where a thin needle is inserted between the ribs into the pleural space, fluid is removed, and the needle is withdrawn. The procedure is performed with ultrasound guidance for safety, takes thirty to sixty minutes, and provides immediate relief of breathing symptoms.
The fluid removed is sent to the laboratory for analysis. The lab examines the cells in the fluid for cancer, measures protein and other chemistries, and may perform additional tests like immunohistochemistry. Cytology of the fluid sometimes confirms mesothelioma directly, though the diagnosis is more often made on tissue biopsy because fluid cytology has variable sensitivity for mesothelioma cells.
Effusion fluid is sent to pathology for cytology and biomarker testing.
The Recurrent Effusion Problem
Effusions in mesothelioma are usually recurrent. Drain them once and they return within days to weeks. Repeated thoracentesis becomes impractical for ongoing care. The patient needs a more durable solution to manage symptoms over time.
Two main options exist. The first is pleurodesis, a procedure that adheres the two layers of pleura together so that no space remains for fluid to accumulate. Talc pleurodesis, performed during a brief surgical procedure called video-assisted thoracoscopic surgery, is the most common. Talc powder is sprayed into the pleural space. Inflammation causes the layers to scar together. Effusions usually do not recur after successful pleurodesis.
The second is an indwelling pleural catheter. A small catheter is placed through the chest wall into the pleural space and tunnelled under the skin to a connection port. The patient or a home health nurse drains the catheter periodically into a vacuum bottle, removing accumulated fluid as needed. The catheter is comfortable to live with and avoids surgery. Over time, the catheter often induces spontaneous pleurodesis, after which it can be removed.
Pleurodesis vs. Indwelling Catheter
Both options manage effusions effectively. The choice depends on the patient’s clinical situation, performance status, and preferences. Patients fit enough for surgery and motivated to avoid an indwelling device often choose pleurodesis. Patients who want to avoid surgery, who are too frail for general anaesthesia, or who prefer the flexibility of intermittent drainage often choose the catheter.
Pleurodesis has approximately a seventy to ninety percent long-term success rate at controlling effusions. The indwelling catheter has similar overall success when measured by symptom relief. The choice is increasingly individualised. Discuss both options with the thoracic team to find the right fit.
When to Drain Asymptomatic Effusions
Not every effusion needs to be drained. Small effusions that do not cause symptoms can sometimes be observed. Drainage carries minor risks including pneumothorax (collapsed lung), bleeding, and infection. The decision to drain weighs symptom severity against procedural risks.
Effusions that compress the lung enough to cause shortness of breath, that are needed for diagnostic sampling, or that interfere with planned imaging studies usually warrant drainage. Asymptomatic small effusions may be left alone, particularly in elderly or frail patients where the risks of intervention outweigh the symptom benefits.
Effusions and Treatment Response
The size and rate of effusion accumulation often track with the underlying disease activity. Effusions that decrease after starting mesothelioma treatment suggest the treatment is working. Effusions that increase suggest disease progression. The pattern is one of several monitoring tools used by the treating team alongside imaging, blood biomarkers, and symptom assessments.
Patients with indwelling pleural catheters can track their daily drainage volumes as a personal monitoring tool. A trend toward less drainage over time is encouraging. A trend toward more drainage warrants discussion with the team and possibly imaging to assess.
A Practical Closing Note
Pleural effusion is one of the most consistently manageable symptoms of pleural mesothelioma. Drainage works. Pleurodesis and indwelling catheters provide durable control. The technology and techniques have improved over decades, and the breathing relief that follows successful management is meaningful for quality of life.
If you are dealing with recurrent effusions, ask your team about pleurodesis or indwelling catheter as the next step. Repeated thoracentesis is appropriate for short-term management but should not be the long-term plan when better options exist.
This article is for educational purposes and does not replace personalised guidance from a pulmonologist or thoracic surgeon.
Your oncologist mentioned the stage of your mesothelioma. Stage I, stage II, stage III, or stage IV. They explained that staging affects treatment options and prognosis. The full staging system uses three letters: T, N, and M. You nodded. You went home. You still are not sure what your stage means.
This guide explains the mesothelioma staging system in plain language. You will learn what T, N, and M each measure, how the four stages combine these factors, what each stage means for treatment, and what survival statistics typically look like at each stage. The goal is to help you understand where your case fits.
Imaging is central to determining T, N, and M categories.
What TNM Means
The TNM system is the standard cancer staging framework used internationally. T stands for tumour and describes how much tumour is present and where it has spread within the chest. N stands for nodes and describes whether and how far the tumour has spread to lymph nodes. M stands for metastasis and describes whether the cancer has spread to distant organs outside the chest.
Each letter is followed by a number indicating extent. T1 to T4 for tumour size and invasion. N0 to N2 for lymph node involvement. M0 or M1 for distant metastases. The combination of T, N, and M values determines the overall stage from I to IV.
T Categories: What the Tumour Has Done
T1 means tumour is limited to the parietal pleura, the chest wall lining, on one side. The lung surface itself is not heavily involved. T2 means tumour has involved the visceral pleura on the lung surface and the diaphragm or lung tissue itself. T3 means tumour has invaded structures in the chest like the chest wall fascia, mediastinal fat, or a single area of chest wall muscle. T4 means tumour has invaded structures that make complete surgical removal impossible: extensive chest wall, the diaphragm with abdominal involvement, the heart, the spine, or the contralateral pleura.
The T category is determined by imaging studies including CT, MRI, and PET scans, sometimes confirmed at surgery. The category drives the surgical decision because T4 disease generally cannot be completely resected.
Multidisciplinary review combines imaging, biopsy, and clinical findings.
N Categories: What the Lymph Nodes Show
N0 means no lymph node involvement. N1 means involvement of nodes within the lung itself or directly adjacent to it on the same side. N2 means involvement of nodes in the mediastinum, the central chest space, on either side. The N category often requires confirmation by lymph node biopsy or surgical sampling because imaging alone cannot reliably distinguish enlarged nodes from normal nodes.
For pleural mesothelioma, lymph node involvement worsens prognosis significantly. Patients being considered for surgery often undergo a procedure called mediastinoscopy or endoscopic ultrasound-guided needle biopsy to sample mediastinal lymph nodes before deciding on surgery. Finding cancer in N2 nodes typically moves the patient out of the surgical category.
M Categories: Has It Spread Distantly
M0 means no distant metastasis. M1 means cancer has spread to distant sites such as the contralateral chest, the bone, the liver, or other distant organs. Distant metastasis is uncommon in mesothelioma compared to other cancers, but when it occurs it changes the treatment approach because curative-intent therapy is no longer feasible.
PET-CT scans are the standard tool for assessing M status. The PET scan shows metabolic activity that distinguishes cancer from non-cancer in distant sites. Positive findings on PET often warrant biopsy confirmation before changing treatment plans, because PET scans have limitations.
Combined Stages I Through IV
Stage IA combines T1 with N0 and M0. Tumour is limited to one side of the parietal pleura with no nodal or distant spread. Stage IB combines T2 or T3 with N0 and M0. Stage II combines T1 or T2 with N1 and M0. Stage IIIA combines T3 with N1 and M0. Stage IIIB includes any T or N when N2 is involved or when T4 is reached, with M0. Stage IV is any T, any N, with M1.
The boundaries are approximate and have been refined over the years. The most current staging system, the AJCC 8th edition, sets out specific criteria. Your medical record should specify the exact T, N, and M values rather than just the overall stage, because the treatment implications depend on the specific combination.
How Stage Affects Treatment
Stage I and II patients are often surgical candidates if other criteria are met. Stage IIIA patients are sometimes surgical candidates with neoadjuvant chemotherapy. Stage IIIB and IV patients are typically not surgical candidates and are managed with systemic therapy, most often the chemotherapy and immunotherapy combinations discussed in other articles. The stage at diagnosis substantially shapes the mesothelioma treatment trajectory.
The cell type also matters. Even at favourable stages, sarcomatoid mesothelioma is treated more conservatively because surgery has not produced strong outcomes. Even at less favourable stages, epithelioid mesothelioma may benefit from aggressive multimodal therapy.
Survival Statistics by Stage
Median survival figures by stage for pleural mesothelioma have shifted upward as treatments have improved. Approximate ranges from current data: stage I, two to three years median survival with multimodal therapy. Stage II, eighteen to twenty-four months. Stage III, twelve to eighteen months. Stage IV, six to twelve months. Long-term survivors exist at every stage, particularly when patients respond well to immunotherapy combinations.
These statistics describe averages, not individual patients. Some patients far exceed median survival. Some fall short. Treatment response, performance status, age, comorbidities, and other factors all influence individual outcomes. Your specific prognosis depends on much more than your stage.
Restaging During Treatment
Stage at diagnosis is sometimes revised during treatment. Imaging during chemotherapy, surgical findings, or new symptoms can lead to revised T, N, or M assessments. The revisions matter because they reframe the treatment plan. Patients who downstage with chemotherapy may become surgical candidates. Patients who upstage may shift toward more palliative goals.
Ask explicitly about restaging at major decision points in your treatment. The team typically performs restaging imaging before deciding on surgery or after each major phase of therapy. The data informs the next decision.
A Final Note
Understanding your stage helps you understand the broader treatment landscape. It also helps you make sense of statistics and survivor stories you may encounter. A stage IV patient cannot be cured by surgery. A stage I patient often can be approached aggressively. The stage frames the conversation.
Ask your oncologist for the explicit T, N, and M values from your most recent imaging. Ask how they translate to overall stage. Ask how the stage shapes the treatment plan. The answers should be specific, not vague. A treating team that can articulate the staging clearly is a team that is paying attention to the details that matter.
This article is for educational purposes and does not replace personalised guidance from a treating oncologist.
You have been diagnosed with mesothelioma. You are facing surgery, chemotherapy, radiation, or immunotherapy. You cannot work. Your family is worried about money. Medical bills are piling up.
You are angry. You should be. You were exposed to asbestos decades ago because companies chose profits over safety. They knew asbestos was dangerous. They had secret documents proving they knew. They hid the truth. They kept selling asbestos. They did not warn you.
Now you have cancer. And they should pay.
The law is on your side. You have the right to file a mesothelioma lawsuit against the companies that caused your illness. You can get money to pay for medical bills, lost wages, pain and suffering, and to support your family.
This guide will walk you through everything you need to know. You will learn who can file a lawsuit, how much money you might receive, how long the process takes, how to find the right mesothelioma attorney, and what to expect every step of the way.
No complicated legal language. No confusion. Just clear, honest information to help you and your family get the justice and compensation you deserve.
Why You Have the Right to Sue
Let us start with the simple explanation.
For decades, companies made and sold asbestos products. They put asbestos in insulation, brakes, gaskets, pipe covering, ceiling tiles, floor tiles, and hundreds of other products. They knew asbestos was dangerous. They had internal documents proving they knew. They hid those documents. They kept selling asbestos. They did not warn workers. They did not warn the public.
That is negligence. That is wrongful conduct. And the law says they must pay for the harm they caused.
You have the right to sue these companies for:
Medical bills (past and future)
Lost wages (past and future)
Pain and suffering
Loss of enjoyment of life
Emotional distress
Punitive damages (to punish the company for bad behavior)
Legal consultation.
Who Can File a Mesothelioma Lawsuit?
You can file a lawsuit if:
You have been diagnosed with mesothelioma, and
Your mesothelioma was caused by asbestos exposure, and
The asbestos exposure came from products made by a company that is still in business (or that has trust funds for victims)
If your loved one died from mesothelioma, you can file a wrongful death lawsuit. The money goes to the spouse, children, or other family members.
What If You Do Not Know Where You Were Exposed?
Many people do not remember every job they ever had. They do not remember every product they worked with. That is okay. A good mesothelioma attorney will help you figure it out.
Your lawyer will ask you questions about your work history. Where did you work? What did you do? What did you see? What did you handle? What tools did you use? What brands do you remember?
From your answers, your lawyer can figure out which products you were likely exposed to and which companies made them. Asbestos lawyers have huge databases of information about where specific asbestos products were used. They have investigators who can find old records and witnesses.
You do not need to remember everything. Your lawyer will help.
What If You Smoked?
Many mesothelioma patients smoked. That does not disqualify you from filing a lawsuit. Asbestos causes mesothelioma regardless of smoking. Smoking does not cause mesothelioma. Only asbestos does.
Your smoking history may come up in the lawsuit. The asbestos companies may try to blame smoking. But a good lawyer knows how to handle this. Mesothelioma is not a smoking-related cancer. You can still get compensation.
Types of Legal Claims
There are two main ways to get compensation for mesothelioma.
Asbestos Bankruptcy Trust Funds
Many asbestos companies went bankrupt because of all the lawsuits. When they went bankrupt, courts required them to set aside money in trust funds for victims. There are over sixty trust funds holding more than thirty billion dollars.
Filing a claim with a trust fund is usually faster than a lawsuit. You do not have to prove that the company was negligent. You just have to prove that you were exposed to their products and that you have mesothelioma.
Trust fund claims typically pay less than lawsuits, but they are more certain and faster.
Lawsuits Against Solvent Companies
Some asbestos companies are still in business. You can sue them directly. Lawsuits can result in larger payouts than trust funds. But they take longer and there is a risk you could lose at trial.
Most Patients Do Both
The best strategy is usually to do both. File trust fund claims to get money quickly. At the same time, file lawsuits against companies that are still solvent. Your lawyer will handle everything.
Courthouse exterior.
How Much Money Can You Get from a Mesothelioma Lawsuit?
This is the question everyone wants answered. The honest answer is that every case is different.
Average Mesothelioma Settlement Amounts
Average settlement: 1millionto2 million
Range of settlements: 500,000to5 million or more
Trial verdicts: Often higher than settlements, sometimes 5millionto10 million or more
Factors That Affect Settlement Amounts
Strength of evidence: How clearly can you prove which company’s product caused your exposure?
Diagnosis: Mesothelioma settlements are typically higher than lung cancer or asbestosis settlements.
Age: Younger patients often receive more because they have lost more potential earning years.
Medical expenses: Higher medical bills lead to higher settlements.
Number of defendant companies: More companies means more potential defendants and higher total compensation.
State where you file: Some states are more favorable to plaintiffs than others.
Your lawyer’s experience: An experienced lawyer gets better results.
Trust Fund Payouts
Trust fund payouts vary by trust fund. Most mesothelioma victims receive 300,000to1 million from trust funds.
What Percentage Does the Lawyer Take?
Most mesothelioma lawyers work on contingency. This means they take a percentage of the money they win for you. Typical contingency fees are 25 to 40 percent.
For example, if your lawyer takes 33 percent and you receive a 1millionsettlement,yougetabout670,000. Your lawyer gets $330,000. You pay nothing upfront. If you lose, you pay nothing.
How Long Does a Mesothelioma Lawsuit Take?
The timeline varies.
Trust fund claims: Usually 6 to 12 months. Some pay faster. Some take longer.
Lawsuits: Usually 12 to 24 months. Some settle faster. Some go to trial and take 2 to 3 years.
Expedited processing: If you have a serious illness, many trust funds and courts will prioritize your case. You can receive compensation much faster.
The Statute of Limitations: Do Not Wait
Every state has a deadline for filing a lawsuit. This is called the statute of limitations.
For personal injury (you are alive): Usually 1 to 4 years from the date you were diagnosed.
For wrongful death (your loved one died): Usually 1 to 4 years from the date of death.
If you miss the deadline, you lose your right to sue forever. That is why you need to call a lawyer as soon as possible. Do not wait.
Why You Should Not Wait Even if You Are Very Sick
Some patients think, “I am too sick to deal with a lawsuit. I just want to focus on treatment.”
We understand. But here is why you should not wait.
The statute of limitations is ticking.
Your lawyer does almost all the work. You will not be stressed with paperwork.
Many patients find that taking legal action gives them a sense of purpose and control.
The money can help your family after you are gone.
Call a lawyer today. You can always decide not to move forward. But you cannot go back in time if you miss the deadline.
How to Find the Best Mesothelioma Attorney
You need a lawyer who specializes in asbestos cases. Do not hire a general personal injury lawyer. Mesothelioma cases are complicated. You need someone who does this work every day.
What to Look For
The best mesothelioma attorney will:
Specialize only in asbestos cases
Have handled hundreds or thousands of mesothelioma cases
Have a track record of large settlements and verdicts
Work on contingency (you pay nothing upfront)
Offer a free consultation
Be willing to travel to you
Questions to Ask Before Hiring a Lawyer
How many mesothelioma cases have you handled?
How much money have you recovered for clients?
Do you handle trust fund claims and lawsuits?
Will you come to me, or do I need to travel to you?
What percentage do you take as your fee?
Do I have to go to court? (Most patients do not.)
Do Not Worry About Location
Do not worry about finding a lawyer in your city. Mesothelioma lawyers work with clients all over the country. They can handle everything by phone, mail, and email. They will come to your home or hospital room to meet with you.
What to Expect in a Mesothelioma Lawsuit
Here is the step-by-step process.
Step One: Free Consultation
You call a lawyer. They ask basic questions. Your diagnosis. Your work history. Your exposure history. They tell you if you have a case. There is no cost.
Step Two: Investigation
Your lawyer investigates your case. They gather your medical records. They take your detailed work history. They identify which companies made the products you were exposed to. They find witnesses and old records.
Step Three: Filing the Claim
Your lawyer files claims with trust funds and/or lawsuits against asbestos companies. This starts the legal process.
Step Four: Discovery
Both sides exchange information. Your lawyer will ask the companies for documents. The companies may ask you questions (written or oral). Your lawyer prepares you for this.
Step Five: Negotiation
Most mesothelioma cases settle without going to trial. Your lawyer negotiates with the companies. They try to reach a fair settlement.
Step Six: Trial (if needed)
If the companies will not offer a fair settlement, your case may go to trial. A jury hears the evidence and decides how much money you get.
Most cases settle. But you want a lawyer who is not afraid to go to trial. Companies offer more money when they know your lawyer will fight.
Step Seven: You Receive Compensation
When your case settles or you win at trial, you receive a check. Your lawyer takes their fee. The rest goes to you.
Mesothelioma Lawsuits for Veterans
If you are a veteran, you have additional options.
VA Benefits
The VA offers disability compensation and free health care for veterans with service-connected mesothelioma. This is separate from lawsuits. You can receive both.
Lawsuits for Veterans
Veterans can also file lawsuits against the companies that made the asbestos products used on ships, in bases, and in vehicles. The Navy did not make asbestos. They bought it from private companies. Those companies can be sued.
The Feres Doctrine
There is a legal rule called the Feres Doctrine. It says that active-duty service members cannot sue the military for injuries that happened during service. But you can sue the companies that made the products. Your lawyer will know how to handle this.
Mesothelioma Lawsuits for Family Members (Secondhand Exposure)
Many people were exposed to asbestos through a family member. A parent who worked in a shipyard brought asbestos fibers home on their work clothes. A spouse who washed those clothes inhaled asbestos. A child who hugged their parent inhaled asbestos.
These family members can also file lawsuits. The law recognizes secondhand exposure as a valid cause of mesothelioma.
Frequently Asked Questions
How much does a mesothelioma lawyer cost? Nothing upfront. Mesothelioma lawyers work on contingency. They only get paid if they win money for you. You pay nothing if you lose.
Do I have to go to court? Most mesothelioma patients never go to court. Their cases settle. If your case does go to trial, you may need to testify. But your lawyer will prepare you. It is not as scary as it sounds.
What if the company that exposed me is out of business? Many asbestos companies are out of business. But when they went bankrupt, they were required to set up trust funds for victims. Your lawyer can file claims with those trust funds.
Can I file a lawsuit if my loved one already passed away? Yes. This is called a wrongful death lawsuit. The money goes to the spouse, children, or other family members.
How long do I have to file a lawsuit? Every state has a deadline called the statute of limitations. It is usually 1 to 4 years from the date of diagnosis or death. Call a lawyer as soon as possible.
Will filing a lawsuit be stressful? Your lawyer does almost all the work. They handle the paperwork, the phone calls, and the negotiations. You focus on your health and your family. Many patients find that taking legal action gives them a sense of purpose and control.
Hope and Action
You have been through so much already. A terrifying diagnosis. Painful treatments. Worry about your family and your finances. You did not ask for any of this.
But here is the truth. The companies that caused your illness owe you. They knew asbestos was dangerous. They hid the truth. They kept selling it anyway. They put their profits ahead of your life.
Now it is time to hold them responsible.
You can get money to pay your medical bills. You can get money to replace your lost income. You can get money to support your family. You can get justice.
Do not wait. Call a mesothelioma attorney today. The call is free. The consultation is free. You pay nothing unless you win.
You served your country. You worked hard. You raised your family. You did everything right. Now it is time for the law to serve you.
Take the first step today.
Disclaimer: This article provides general information about mesothelioma lawsuits, legal rights, and settlements. It does not constitute legal advice. Every case is different. Laws vary by state. Statutes of limitations vary. Always consult with a qualified mesothelioma attorney about your specific situation. If you or a loved one has been diagnosed with mesothelioma, speak with a doctor immediately and contact a qualified mesothelioma lawyer to understand your legal rights. Do not wait. Deadlines apply. Your family is counting on you.
Imaging suggested mesothelioma. The next step is a biopsy. Your team mentioned several options: a needle through the chest wall, a small surgical procedure called VATS, or a more invasive operation. The vocabulary is unfamiliar. The decision feels weighty.
This guide explains mesothelioma biopsy procedures in plain language. You will learn the three main biopsy approaches, when each is used, what to expect during and after each, and why getting tissue from the right location matters for diagnostic accuracy.
Mesothelioma diagnosis requires adequate tissue for pathology and biomarker testing.
Why Biopsy Is Necessary
Imaging studies and pleural fluid analysis can suggest mesothelioma but cannot definitively diagnose it. The diagnosis requires tissue examined under a microscope by a pathologist who confirms the cell pattern, performs immunohistochemistry to rule out other cancers, and identifies the specific mesothelioma subtype. Without tissue, treatment cannot proceed.
The amount of tissue matters. Small biopsies sometimes show suspicious findings that cannot be definitively classified. Larger biopsies allow more comprehensive testing including molecular studies that may identify treatment-relevant mutations. Whenever possible, the goal is a tissue sample large enough for full diagnostic and biomarker analysis.
Image-Guided Needle Biopsy
The least invasive option is a needle biopsy performed through the chest wall under CT or ultrasound guidance. An interventional radiologist places a thin needle into the area of pleural thickening and removes small core samples of tissue. The procedure is outpatient, takes thirty to sixty minutes, and uses local anaesthesia.
Needle biopsy is often appropriate when imaging shows clear pleural thickening that can be safely accessed. The advantages are the minimal invasiveness, quick recovery, and outpatient delivery. The limitations are the smaller tissue sample, occasional sampling errors that miss the cancer, and difficulty accessing some areas of the pleura. Successful diagnostic yield is roughly seventy to eighty percent for experienced operators.
Video-Assisted Thoracoscopic Surgery (VATS)
VATS is a minimally invasive surgical procedure performed under general anaesthesia. The surgeon makes two or three small incisions in the chest, inserts a camera and instruments, and directly visualises the pleural surfaces. Biopsies are taken under direct vision from the most suspicious areas. Pleurodesis can be performed at the same operation if appropriate.
VATS is the diagnostic procedure of choice at most mesothelioma treatment centers when needle biopsy is not feasible or when a larger tissue sample is needed. The diagnostic yield exceeds ninety-five percent. The procedure is also therapeutic when combined with talc pleurodesis or fluid drainage. Hospital stay is typically one to two days.
Imaging guides biopsy targeting; VATS allows direct surgical visualisation.
Open Surgical Biopsy
Open surgical biopsy through a thoracotomy incision is uncommon today but remains an option in specific circumstances. It may be used when VATS is not feasible due to dense pleural adhesions, when more extensive tissue is needed for research protocols, or when the diagnostic plan also includes major resection at the same operation. The procedure involves a larger incision, longer recovery, and more pain than VATS.
For most patients, the diagnostic question can be answered without resort to open biopsy. Modern minimally invasive techniques have largely replaced open biopsy for diagnostic purposes alone.
What Happens to the Tissue
The pathologist receives the tissue, processes it in formalin, embeds it in paraffin, and prepares thin slices on glass slides. Stains highlight cellular features. Immunohistochemistry uses antibodies to detect specific proteins that distinguish mesothelioma from other cancers. The standard mesothelioma panel typically includes calretinin, WT-1, CK5/6, and others as positive markers, plus several markers used to rule out lung adenocarcinoma and other cancers.
The pathologist also classifies the cell type. Epithelioid mesothelioma has a more uniform appearance and better prognosis. Sarcomatoid mesothelioma has a spindle-cell appearance and worse prognosis. Biphasic mesothelioma combines both patterns. The classification matters for treatment selection and for survival prediction.
Second-Look Pathology
Mesothelioma diagnosis is challenging even for experienced pathologists. A second-look review by a pathologist with mesothelioma expertise can refine the diagnosis or occasionally reverse it. Specialty centres routinely perform second-look pathology when patients arrive from outside institutions. The investment is worthwhile because misdiagnosis happens and the treatment implications are major.
If your local pathology report is uncertain or if you are seeking specialty-centre care, request that the slides be sent for review. The slides remain the institution’s property after preparation, and copies or the originals can be transferred for outside consultation.
Recovery After Biopsy
Needle biopsy recovery is brief. Most patients go home the same day, with mild incisional discomfort that resolves over a few days. Pneumothorax, a small lung collapse, is a possible complication and may require a brief observation period. Bleeding and infection are rare.
VATS recovery is more substantial. Hospital stay is typically one to two days. Chest tube placement during the procedure manages air and fluid drainage. Tube removal usually occurs on day one or two when the lung is fully expanded and drainage has stopped. Pain is managed with oral medications. Most patients return to normal activity within two to three weeks.
Practical Closing Notes
The biopsy method should be chosen by a multidisciplinary team that considers your imaging, your overall fitness, and the diagnostic question being asked. Most patients today receive VATS-based biopsies because the diagnostic yield is so high and the procedure is well-tolerated.
Whatever method is used, plan for the diagnostic phase to take a few weeks from imaging to definitive pathology report. The waiting is hard. Use the time to schedule consultations at specialty centres so that treatment planning can begin as soon as the diagnosis is confirmed.
This article is for educational purposes and does not replace personalised guidance from a thoracic surgeon or pathologist.
Mesothelioma diagnosis and monitoring rely heavily on imaging. CT scans, MRI, and PET scans each have specific roles. Knowing what each test does, when it is ordered, and what the radiologist is looking for helps you understand your care.
This guide explains mesothelioma imaging tests in plain language. You will learn how CT, MRI, and PET differ, when each is used, what preparation is required, and how they fit into the larger picture of staging and monitoring.
Imaging studies guide diagnosis, staging, surgical planning, and treatment monitoring.
CT Scan: The Foundation
The CT scan, also called a computed tomography scan, is the first and most frequent imaging study in mesothelioma. CT uses X-rays from multiple angles, processed by a computer into cross-sectional images of the chest. The scan shows pleural thickening, pleural effusion, lung involvement, mediastinal lymph nodes, and chest wall invasion in fine anatomical detail.
A chest CT with contrast is the standard for mesothelioma. The contrast is an iodine-based dye injected through a vein during the scan. The dye enhances vascular structures and tumour, making them stand out from normal tissue. Patients with kidney problems or contrast allergies use modified protocols. The scan itself takes a few minutes; the entire appointment is typically thirty to sixty minutes.
CT is used for initial diagnosis, staging, surgical planning, response assessment during treatment, and surveillance after treatment. Typical surveillance schedules involve CT every three to four months for the first year or two, with longer intervals thereafter if the disease is stable.
MRI: When CT Is Not Enough
MRI uses magnetic fields and radio waves rather than X-rays. The images excel at distinguishing soft tissue types, including the boundary between tumour and normal structures like the diaphragm muscle, the heart, and the chest wall. For surgical planning, MRI sometimes adds detail that CT alone cannot provide.
MRI is particularly useful when CT is ambiguous about whether tumour has invaded specific structures. Diaphragm involvement, mediastinal invasion, and chest wall infiltration can sometimes be better assessed with MRI. The cost and longer scanning time mean MRI is reserved for situations where the additional detail will change management.
CT and MRI provide complementary anatomical detail; PET adds metabolic information.
PET-CT: Metabolic Information
PET-CT combines a CT scan with a metabolic imaging study using a radioactive sugar called FDG. Cancer cells take up the FDG more avidly than normal cells because they consume more energy. The PET image highlights areas of high metabolic activity, which usually correspond to active tumour.
For mesothelioma, PET-CT is used most often for initial staging to assess for distant metastases that might not be visible on CT alone. PET helps detect lymph node involvement, contralateral chest disease, and unsuspected sites elsewhere in the body. PET findings often prompt additional biopsy to confirm metastatic disease before changing treatment plans.
PET-CT is also used during treatment to assess response. Tumours that are responding to therapy show decreased FDG uptake. Tumours that are progressing show increasing uptake. The metabolic information complements the anatomical information from CT and helps distinguish active tumour from post-treatment scarring or fibrosis.
What Preparation Is Required
CT with contrast requires fasting for several hours before the scan and adequate hydration before and after. If you have kidney problems, your doctor may order a creatinine blood test before the scan to verify it is safe to receive contrast. Metformin diabetes medication is sometimes held before and after contrast administration.
MRI requires removal of all metal objects, including jewellery and clothing with metal fasteners. Patients with pacemakers, certain stents, or other implanted metal devices may not be eligible for MRI. The scan involves lying still in a tube for thirty to sixty minutes. Patients with claustrophobia can request a mild sedative.
PET-CT requires fasting for four to six hours before the scan because food affects sugar uptake by the radioactive tracer. After receiving the FDG injection, you wait quietly for about an hour while the tracer distributes through the body. The scan itself takes approximately thirty minutes.
Reading the Reports
Imaging reports follow a standard format. The radiologist describes the findings region by region: pleura, lungs, mediastinum, chest wall, upper abdomen. They note the size and characteristics of any tumour, comparing to prior studies when available. They give an impression summarising the key findings.
Common terms in mesothelioma reports include rind-like pleural thickening, nodular pleural enhancement, pleural effusion, septations, fissural extension, mediastinal lymphadenopathy, and trans-diaphragmatic extension. Ask your oncologist to walk you through the report at your next visit. Understanding what the radiologist saw helps you understand the treatment recommendations that follow.
Imaging During Treatment
Imaging during treatment monitors response. The standard interval for CT during chemotherapy is every two to three cycles, typically every six to nine weeks. The CT looks for change in pleural thickening, change in effusion size, and any new sites of disease. The findings inform whether to continue, modify, or change the treatment.
After completion of curative-intent treatment, surveillance imaging continues every three to four months for the first two years, then every six months for several more years. Most recurrences are detected on imaging before symptoms develop, which sometimes allows earlier treatment of progression.
A Closing Note
Imaging is a constant companion through mesothelioma treatment. Each scan can produce anxiety while waiting for results. The waiting is hard but unavoidable. Most patients develop a routine of scan, follow-up appointment, decision, repeat. The information from each scan informs the next phase.
Ask your oncologist what they are looking for at each scan and what specific findings would change the treatment plan. The answers help you understand which aspects of the report matter most and which are routine. The knowledge replaces some of the uncertainty with clarity.
This article is for educational purposes and does not replace personalised guidance from a treating oncologist or radiologist.
Blood tests are a familiar part of medical care. Most patients expect them. For mesothelioma, certain blood tests can support diagnosis, monitor disease, and complement other tests, though no single blood test confirms or rules out the disease on its own.
This guide explains the mesothelioma blood tests and biomarkers used in clinical practice today. You will learn what each test measures, what its strengths and limitations are, and how it fits into the broader diagnostic and monitoring picture.
Mesothelioma biomarkers are tools, not standalone diagnostic tests.
Mesomark and Soluble Mesothelin-Related Peptide
The most established mesothelioma blood biomarker is soluble mesothelin-related peptide, abbreviated SMRP. Mesothelin is a protein expressed on mesothelial cells. Mesothelioma tumours often shed mesothelin into the bloodstream, where it can be measured. The Mesomark test is the FDA-approved assay for SMRP.
Elevated SMRP supports a mesothelioma diagnosis when other findings are suspicious. Lower levels do not rule out mesothelioma because some tumours, particularly sarcomatoid types, do not produce mesothelin. The test is most useful as part of a panel including imaging, biopsy, and other markers, not as a standalone test.
SMRP can also track disease activity over time. Decreasing levels during treatment suggest response. Rising levels can suggest progression and may prompt restaging imaging earlier than the routine schedule.
Fibulin-3
Fibulin-3 is another biomarker that has shown elevation in pleural mesothelioma. Studies have evaluated it both in blood and in pleural fluid. The diagnostic accuracy varies across studies. Fibulin-3 is not as widely used as SMRP and is not FDA-approved as a standalone diagnostic test, but it is sometimes measured alongside SMRP at major research centres.
The combination of multiple biomarkers may improve diagnostic accuracy beyond any single marker. Research continues to refine the optimal panel.
Osteopontin and Megakaryocyte Potentiating Factor
Two other biomarkers studied in mesothelioma are osteopontin and megakaryocyte potentiating factor, or MPF. Both have shown some diagnostic utility in research settings. Neither has reached widespread clinical use comparable to SMRP. Specialty centres may include them in panels for specific diagnostic situations.
The history of biomarker development for mesothelioma reflects the difficulty of finding markers that are sensitive enough to catch early disease and specific enough to avoid false positives. None of the available markers fully solves both problems.
Biomarker results inform but do not replace clinical and pathological diagnosis.
Standard Blood Tests Routinely Ordered
Beyond mesothelioma-specific biomarkers, several routine blood tests are ordered throughout treatment. Complete blood count tracks red cells, white cells, and platelets, which are all affected by chemotherapy. Comprehensive metabolic panels track kidney and liver function. These tests are drawn at every cycle of chemotherapy and are essential for safe treatment delivery.
Tumour markers from other cancer panels, like CA 125 or carcinoembryonic antigen, may be elevated in some mesothelioma patients but are not specific for the disease. They are sometimes used as monitoring tools when their initial level was clearly elevated.
Liquid Biopsy and Circulating Tumour DNA
The frontier of mesothelioma blood-based diagnostics is liquid biopsy, which uses blood samples to detect circulating tumour DNA. The DNA fragments released by dying tumour cells can be analysed for cancer-specific mutations. Liquid biopsy is increasingly used in many cancers for monitoring response, detecting resistance mutations, and identifying minimal residual disease after treatment.
For mesothelioma, liquid biopsy applications are still developing. The technology is being studied for monitoring response to immunotherapy, detecting recurrence early, and identifying patients who would benefit from specific targeted therapies. Patients at major centres may have liquid biopsy performed as part of clinical trials or research protocols.
Insurance and Cost
The Mesomark test for SMRP is generally covered by major insurers when ordered for an appropriate clinical indication. Coverage for newer biomarkers and liquid biopsy applications varies more widely. Out-of-pocket costs for niche tests can range from several hundred to several thousand dollars when not covered.
Always verify coverage before tests are ordered, particularly for non-standard panels. Specialty centres often handle the verification but it is worth confirming. Surprise lab bills are a common source of frustration in cancer care.
A Realistic Note on Limitations
Despite years of research, no blood test today is sensitive and specific enough to diagnose mesothelioma without imaging and biopsy. The biomarkers we have are useful adjuncts. They are not replacements. Anyone offering a “mesothelioma blood test that confirms diagnosis” without other workup is overselling the technology.
That said, biomarkers add real information when used alongside other tests. Trends over time can be informative. Initial values can support clinical impressions. The thoughtful integration of blood-based and imaging-based tests is part of high-quality mesothelioma treatment at experienced centres.
Closing Note
Ask your oncologist which blood-based tests they routinely use in your monitoring plan and what changes in those values would prompt action. The answers help you participate in your own care. They also help you avoid unnecessary anxiety about minor fluctuations that are not clinically significant.
The field is evolving. New tests are coming. The biomarker landscape for mesothelioma in 2030 will likely look different than today’s. For now, the established tools described above represent the practical state of the art.
This article is for educational purposes and does not replace personalised guidance from a treating oncologist.
The early symptoms of mesothelioma can look almost identical to lung cancer. Cough. Shortness of breath. Chest pain. Weight loss. Fatigue. Even the imaging findings overlap. Distinguishing the two diseases requires careful pathology and clinical assessment, and the distinction matters because the treatments differ significantly.
This guide explains how doctors tell the difference between mesothelioma vs lung cancer. You will learn the differences in tumour biology, growth pattern, imaging appearance, and pathology that allow accurate diagnosis. Understanding the distinction helps you understand your own diagnosis and treatment plan.
Mesothelioma grows on the lung lining; lung cancer grows from lung tissue itself.
Different Cells of Origin
The fundamental difference is the cell of origin. Lung cancer arises from cells in the lung tissue itself, most commonly the lining of airways or the alveolar cells where gas exchange occurs. Mesothelioma arises from mesothelial cells that line the pleural cavity surrounding the lungs. The lung itself is healthy tissue; the disease is in the lining around it.
This difference shapes how each disease grows. Lung cancer typically forms a discrete tumour mass within the lung. Mesothelioma typically grows as a diffuse sheet across the pleural surface, sometimes with multiple nodules but rarely as a single isolated mass. The pattern is visible on imaging and at surgery.
Different Causes
Lung cancer is most often caused by tobacco smoking. Other contributors include radon exposure, occupational exposures to certain chemicals, and family history. Some lung cancers occur in non-smokers and may have specific genetic drivers.
Mesothelioma is caused almost exclusively by asbestos exposure. The latency period from asbestos exposure to diagnosis is typically twenty to fifty years. Patients often had occupational exposure decades ago in industries like shipbuilding, construction, automotive brake repair, or insulation work. Family members exposed to asbestos brought home on workers’ clothing can also develop mesothelioma. Smoking does not cause mesothelioma but does increase the risk of lung cancer in asbestos-exposed individuals.
Imaging patterns differ but can overlap; pathology is the definitive distinction.
Imaging Differences
On chest CT, lung cancer typically appears as a discrete mass within the lung tissue, sometimes with associated lymph node enlargement and possibly distant metastases. The lung tissue around the tumour may show signs of obstruction. Mesothelioma typically appears as thickening of the pleural surface, often circumferential around the lung, frequently with pleural effusion. The lung itself often looks compressed but otherwise structurally normal.
Some patterns blur. A lung cancer can invade the pleura and produce pleural thickening. A mesothelioma can occasionally form a discrete mass. The radiologist looks at the dominant pattern, the asymmetry, the distribution, and other features to lean one way or the other. The final answer comes from pathology.
Pathology Distinguishes the Two
Tissue examination by a pathologist is the definitive test. Lung adenocarcinoma is the most common lung cancer and is the one most often confused with mesothelioma on initial appearance. Both can show glandular patterns under the microscope. Immunohistochemistry, however, distinguishes them clearly in most cases.
Mesothelioma typically expresses calretinin, WT-1, CK5/6, and other mesothelial markers. Lung adenocarcinoma typically expresses TTF-1, napsin A, and other lung lineage markers. The pattern of staining usually identifies the cell type with high confidence. Difficult cases may require additional studies, but most diagnoses can be made on the standard panel.
Sarcomatoid mesothelioma poses a particular challenge because its appearance can mimic spindle-cell carcinomas of various origins. The immunohistochemical panel is broader for sarcomatoid cases, and second-look pathology by a mesothelioma expert is sometimes essential.
Why the Distinction Matters for Treatment
Lung cancer treatment depends on cell type and stage but typically involves surgery for localised disease, often combined with chemotherapy and radiation. Targeted therapies for specific genetic mutations have transformed outcomes for some lung cancers. Immunotherapy is also widely used.
Mesothelioma treatment differs significantly. Surgery is more limited and uses different operations like P/D and EPP. The chemotherapy backbone is different, with cisplatin and pemetrexed being the standard. Immunotherapy is increasingly important. The targeted therapy landscape is much smaller than for lung cancer because mesothelioma has fewer well-characterised driver mutations.
Misdiagnosing mesothelioma as lung cancer or vice versa leads to inappropriate treatment. Patients treated for the wrong disease miss the chance to receive the most effective therapies for what they actually have. Confirming the diagnosis carefully, with second-look pathology when there is any doubt, is worth the extra time.
Why the Distinction Matters for Compensation
For asbestos-exposed patients, the distinction also matters for compensation. Mesothelioma is the signature disease of asbestos exposure and is qualifying for asbestos trust fund claims and many state-specific compensation programmes. Lung cancer in asbestos-exposed workers can also be compensable but requires more documentation linking the cancer to asbestos.
If you have been diagnosed with mesothelioma, the legal pathway is generally clearer than for lung cancer alone. The pathology confirmation and the asbestos exposure history together support claims. Documentation of both is important.
Closing Note
Mesothelioma and lung cancer can look similar on initial presentation but are distinct diseases with different causes, growth patterns, treatments, and compensation pathways. The pathology report is the document that locks in the diagnosis. Read it carefully. If anything seems uncertain, request second-look pathology before treatment proceeds.
For patients with significant asbestos exposure history, knowing the difference also matters for legal documentation. Whichever disease you have, accurate diagnosis is the foundation for everything that follows.
This article is for educational purposes and does not replace personalised guidance from a treating oncologist or pathologist.
Your pathology report uses a word that puzzled you. Sarcomatoid. Or epithelioid. Or biphasic. The oncologist explained that this is the cell type, that it affects how aggressive the cancer is, and that it shapes treatment decisions. You did not catch all the implications.
This guide explains the three mesothelioma cell types in plain language. You will learn what each type looks like, what each means for treatment, what the prognosis differences are, and why the cell type might be the single most important feature in your pathology report.
Cell type is determined under the microscope by an experienced pathologist.
Epithelioid Mesothelioma
Epithelioid is the most common cell type, accounting for roughly sixty to seventy percent of mesothelioma cases. Under the microscope, epithelioid mesothelioma cells appear relatively uniform, polygonal, and arranged in patterns that can resemble glandular tissue. The growth tends to be more orderly than the other cell types.
Epithelioid mesothelioma carries the most favourable prognosis among the three types. Median survival ranges from eighteen months to three or more years depending on stage and treatment. Patients with epithelioid disease are the strongest candidates for aggressive multimodal treatment including surgery. The response to chemotherapy and immunotherapy is generally better than for the other types.
Sarcomatoid Mesothelioma
Sarcomatoid is the least common cell type, accounting for ten to twenty percent of cases. Under the microscope, sarcomatoid cells are spindle-shaped, less differentiated, and grow in disorganised patterns. The biology is more aggressive than epithelioid disease.
Sarcomatoid mesothelioma has historically had the most challenging prognosis. Median survival is shorter, often six to twelve months, although immunotherapy combinations have improved outcomes recently. Patients with sarcomatoid disease have generally been considered poor surgical candidates because surgery alone has not produced strong outcomes. Chemotherapy response is more limited than for epithelioid disease.
The recent good news is that sarcomatoid mesothelioma seems to respond particularly well to immunotherapy. The CheckMate 743 trial showed that the survival benefit of nivolumab-ipilimumab compared to chemotherapy was largest in the sarcomatoid and biphasic subgroups. This has changed practice. Patients with sarcomatoid mesothelioma are now strongly considered for first-line immunotherapy.
Treatment selection differs by cell type, especially for surgery and immunotherapy.
Biphasic Mesothelioma
Biphasic mesothelioma combines features of both epithelioid and sarcomatoid cell types in the same tumour. Pathologists report the percentage of each component when documenting biphasic disease. The relative proportions affect prognosis. Tumours that are predominantly epithelioid behave more like epithelioid disease. Tumours that are predominantly sarcomatoid behave more like sarcomatoid disease.
Biphasic mesothelioma represents twenty to thirty percent of cases. The intermediate biology means the prognosis sits between the other two types, but the variation is large depending on cell-type proportions. Treatment selection takes the proportion into account.
Why the Cell Type Matters for Surgery Decisions
Surgical candidacy is heavily influenced by cell type. Epithelioid patients are routinely considered for surgical resection if other criteria are met. Sarcomatoid patients are usually not surgical candidates because surgery alone has not produced meaningful long-term survival in this group. Biphasic patients are evaluated case by case based on the cell-type proportions and other features.
This pattern reflects the underlying biology. Surgery removes localised disease but cannot address microscopic spread that occurs early in aggressive sarcomatoid tumours. For epithelioid disease, where the biology is more contained, surgery has a meaningful role.
Why the Cell Type Matters for Chemotherapy
Chemotherapy with cisplatin and pemetrexed produces meaningful responses in most epithelioid patients but smaller responses in sarcomatoid patients. The difference reflects the cellular biology and the speed of disease progression. Treatment plans for sarcomatoid patients have shifted toward immunotherapy as first-line therapy in many cases, with chemotherapy reserved or used in combination.
Why the Cell Type Matters for Immunotherapy
The pattern with immunotherapy reverses the historical disadvantage of sarcomatoid disease. The nivolumab-ipilimumab combination produces particularly strong responses in sarcomatoid and biphasic mesothelioma compared to chemotherapy. For these subgroups, immunotherapy first-line is now the preferred approach for unresectable disease.
For epithelioid mesothelioma, the choice between chemotherapy first or immunotherapy first is more nuanced. Both produce meaningful responses. Combination protocols using chemotherapy plus immunotherapy are being investigated to maximise response rates.
Why Second-Look Pathology Matters
Cell-type classification can be challenging, particularly for biphasic tumours where the proportions need to be carefully estimated and for sarcomatoid tumours that mimic other spindle-cell cancers. A second-look pathology review by a mesothelioma-experienced pathologist sometimes refines the classification or even changes the diagnosis.
If your cell type was initially classified ambiguously, or if the local pathologist sees few mesothelioma cases per year, ask whether second-look pathology at a specialty centre would be useful. The classification affects treatment decisions, and getting it right is worth the extra step.
Closing Note
Knowing your cell type is essential to understanding your treatment plan and prognosis. The numbers and survival statistics that apply to mesothelioma overall do not necessarily apply to your specific cell type. Ask your oncologist for the precise cell type and, in biphasic cases, the percentage of each component. Use this information to ask sharper questions about treatment decisions and expected response.
The cell type is not destiny. Treatment options exist for every cell type. The right plan for sarcomatoid disease looks different from the right plan for epithelioid disease, but both can produce meaningful survival when treatment is matched to biology.
This article is for educational purposes and does not replace personalised guidance from a treating oncologist or pathologist.
Manage Consent
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.